CRITICAL - Refractory Septic Shock
The hematological profile reflects an acute collapse in coagulation mechanics and advanced toxemia mandating sweeping, aggressive empirical intervention.
Clinical Deviations Paradigm
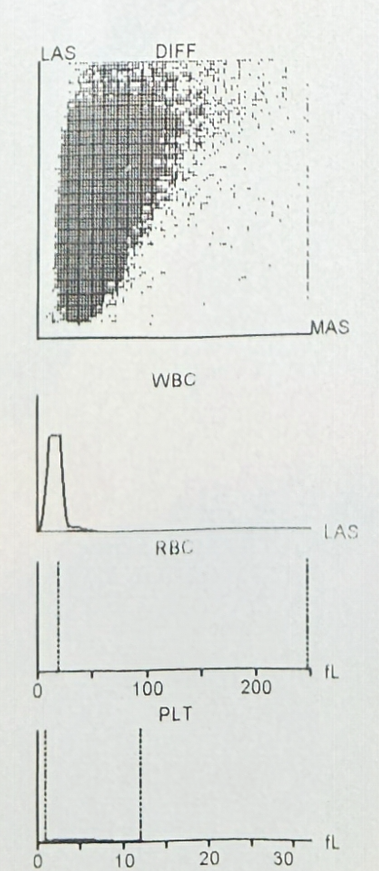
* Data is mapped on a Logarithmic Scale due to catastrophic value disparity.
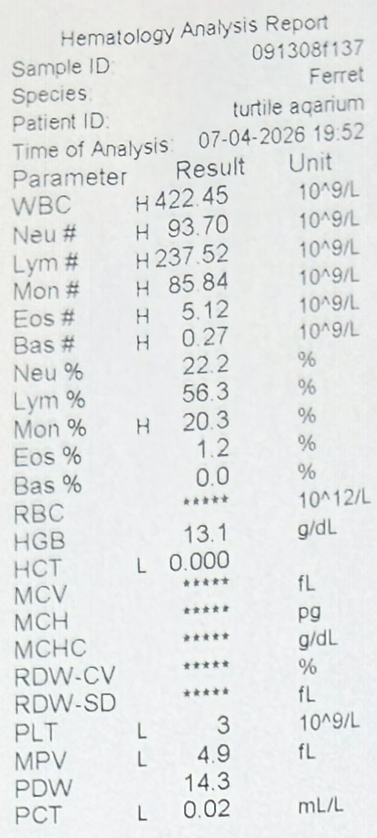
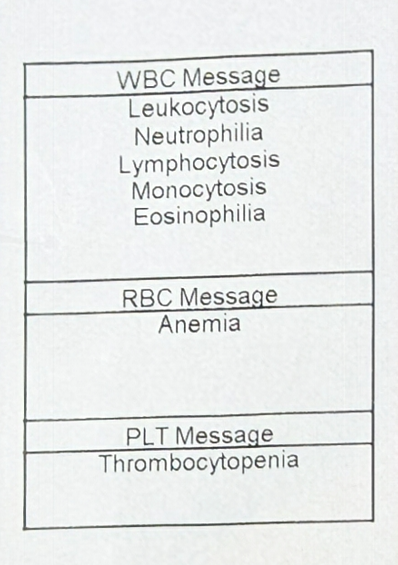
1. White Blood Cells (WBC)
This value is catastrophically elevated (Severe Leukocytosis). In marine turtles, baseline sits between 5 and 15. A surge to 422 yields unequivocal proof of:
-
❖
Leukemoid Reaction & Fulminant Septicemia: A leukemia-mimicking response indicating immense bacterial flooding of the vascular tract, overwhelming endotoxin clearance by the liver and spleen.
2. Platelets (PLT)
Platelet depletion to 3 (near-total absence/Severe Thrombocytopenia) suggests:
Disseminated Intravascular Coagulation. Coagulation factors and fibrinogen are completely exhausted in response to rampant pro-inflammatory cytokines, causing generalized hemorrhagic effusion and sub-scute pooling.
3. Hematocrit (HCT)
A hallmark of Acute Hemolytic & Hemorrhagic Crisis. Attributed to widespread ischemia, red blood cell destruction via bacterial hemolysins, and severe hypovolemic hemodilution.
Clinical Conclusion
The hematological blueprint confirms the subject is embroiled in Decompensated Septic Shock. Laboratory flags broadcast 'Multi-Organ Failure' accompanied by profound physiological devastation.
Mandatory Target Intervention
Clinical tier falls under 'Moribund State'. Emphatic and instantaneous maneuvers are mandatory: Intramuscular Ceftazidime flanked by drastic circulatory volume restitution (Fluid Resuscitation). Survival solely rides on an extreme pharmacokinetic triumph in restoring hemodynamics.
Original Assays Documentation